SURPASS-2- Tirzepatide vs Semaglutide in Type 2 Diabetes



Key Summary: In addition to meeting the primary objective of noninferiority to semaglutide in type 2 diabetes (T2D), tirzepatide, at a dose of either 10 mg or 15 mg once weekly, has demonstrated superiority to semaglutide in this indication. Additionally, tirzepatide was associated with a clinically and statistically significant reduction in body weight compared with semaglutide,...
Key Summary:
In addition to meeting the primary objective of noninferiority to semaglutide in type 2 diabetes (T2D), tirzepatide, at a dose of either 10 mg or 15 mg once weekly, has demonstrated superiority to semaglutide in this indication. Additionally, tirzepatide was associated with a clinically and statistically significant reduction in body weight compared with semaglutide, with achievements of glycated hemoglobin (HbA1c) close to normoglycemia, with 51% of patients reaching a target HbA1c of <5.7% at 40 weeks at a tirzepatide dose of 15 mg once weekly.
Introduction:
Tirzepatide (Mounjaro®) is a highly selective and long-acting dual glucose-dependent insulinotropic polypeptide (GIP) and glucagonlike peptide-1 (GLP-1) receptor agonist1. GLP-1 receptor agonists act by stimulating insulin secretion, suppressing glucagon secretion, delaying gastric emptying, decreasing appetite, and decreasing body weight and have been shown to be effective in the treatment of T2D.2 The incretin hormone GIP acts to increase insulin secretion during hyperglycemia and to increase glucagon levels during fasting and hypoglycemia conditions.3
Tirzepatide is indicated for the treatment of insufficiently controlled T2D in adults, with recommended maintenance doses of 5 mg, 10 mg and 15 mg once weekly, administered by subcutaneous (SC) injection at any time of the day, with or without meals.1 In the SURPASS-2 study, patients were randomized to one of three tirzepatide arms: 5 mg, 10 mg or 15 mg once weekly, or to the active comparator, semaglutide 1mg once weekly, all on a background of metformin.4
Semaglutide is a selective GLP-1 receptor agonist, approved for the treatment of T2D at a maximum dose of 2 mg injected SC once weekly (at the time of the SURPASS-2 study, the maximum approved dose of semaglutide was 1 mg/week).5
“This was an exciting study that was published recently in the New England Journal of Medicine and it was the first time we had compared tirzepatide with a GLP-1 agonist (semaglutide) in people with T2D.”
Figure 1 shows the design of the SURPASS-2 study 1,4
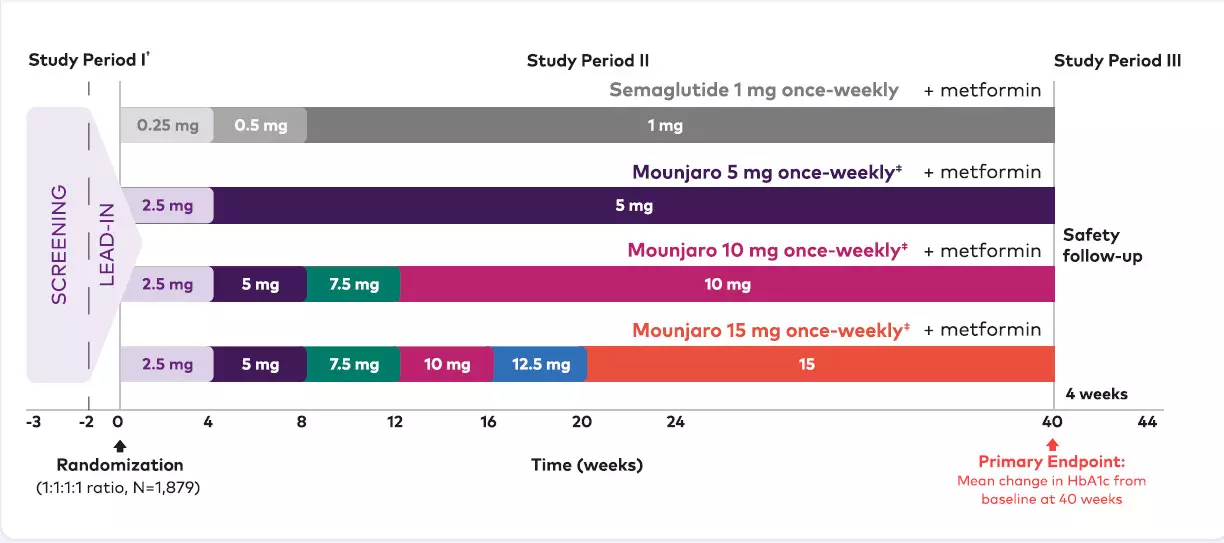
*Patients with T2D who had inadequate glycemic control on stable doses of metformin alone to receive once-weekly SC tirzepatide 5 mg, 10 mg, 15 mg, or once-weekly SC semaglutide 1 mg (1:1:1:1 ratio), all in combination with metformin ≥1500 mg/day.
†Stable doses of metformin ≥1500 mg/day for at least 3 months prior to Visit 1 and during the screening/lead-in period.
‡All tirzepatide doses were double-blinded HbA1c = glycated hemoglobin; SC = subcutaneous; T2D = type 2 diabetes.
The objective of the SURPASS-2 study was to demonstrate that tirzepatide used at a dose of 10mg or 15 mg once weekly was noninferior to semaglutide 1 mg once weekly, the highest licensed dose available for the management of T2D at the time of SURPASS-2.4
The primary endpoint of SURPASS-2 was change in HbA1c from baseline to 40 weeks.4
Key secondary endpoints included4:
- Noninferiority of tirzepatide 5 mg once weekly to semaglutide 1 mg once weekly for glycemic control at 40 weeks.
- Mean change from baseline in HbA1c.
- Superiority of tirzepatide 5 mg, 10 mg and/or 15 mg once weekly to semaglutide 1 mg once weekly at 40 weeks for:
- Mean change from baseline in body weight.
- Mean change from baseline in HbA1c.
- Proportion of patients with HbA1c target values of <7.0%.
- Superiority of tirzepatide 10 mg and/or 15 mg once weekly to semaglutide for the proportion of patients with HbA1c target values of <5.7% at 40 weeks.
Who was in SURPASS-2?
The SURPASS-2 study included a total of 1878 patients with T2D who were receiving a background of metformin therapy, with an HbA1c of ≥7.0% to ≤10.5%, and were randomized to one of the four treatment arms.4 At baseline, the mean age of patients was 56.6years, with a mean HbA1c of 8.3%, characteristic of such trials in patients with T2D, a mean diabetes duration of 8.6 years, and a mean body mass index (BMI) of 34 kg/m2 (Table 1).
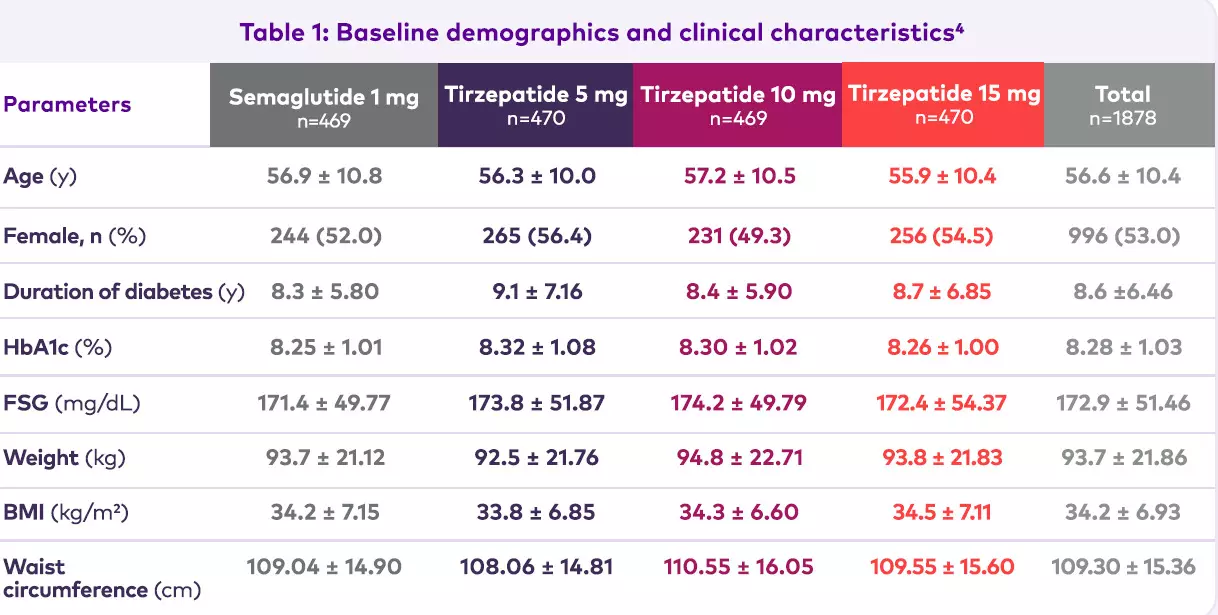
Note: data are mean ± SD unless otherwise specified; mITT population.
BMI = body mass index; FSG = fasting serum glucose; HbA1c = glycated hemoglobin; mITT = modified intent-to-treat;
SD = standard deviation.
Patient disposition
Of the 471 patients randomized to tirzepatide 5 mg once weekly, 431 (91.5%) completed the study still receiving the study drug, with corresponding figures for the 10 mg and 15 mg once-weekly arms of 411/469 (87.6%) and 408/470 (86.8%), respectively, and 428/469 (91.3%) for the semaglutide arm.
Primary endpoint: change in HbA1c
Tirzepatide was associated with greater change from baseline at 40 weeks in HbA1c than semaglutide, with decreases of 2.1%, 2.4% and 2.5%, for tirzepatide 5 mg, 10 mg and 15 mg once weekly, respectively, compared with 1.9% for semaglutide 1 mg once weekly all (p<0,001; Figure 2).
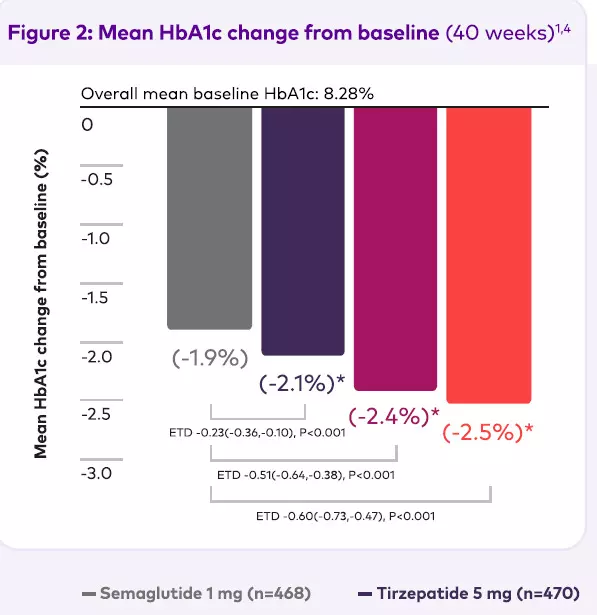
*P<0.001 vs. semaglutide 1 mg for superiority, adjusted for multiplicity. Efficacy estimand. MMRM analysis, mITT population (efficacy analysis set). Data presented are LS mean.
Tirzepatide vs. semaglutide 1 mg at 40 weeks.
HbA1c=glycated hemoglobin; ETD=estimated treatment
difference; LS=least squares; mITT=modified intent-to-treat;
MMRM=mixed model for repeated measures.
All three doses of tirzepatide showed a significantly greater reduction in HbA1c than semaglutide.4
Moreover, the reductions in HbA1c with tirzepatide were seen as early as Week 4 and then continued through to Week 40 (Figure 3).
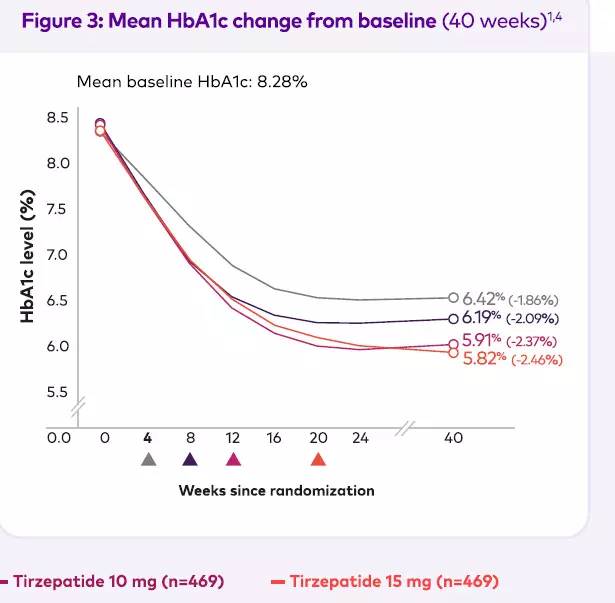
P<0.001 for all tirzepatide doses vs. semaglutide, adjusted for multiplicity. Triangles indicate the times at which the maintenance doses of tirzepatide (5 mg, 10 mg, or 15 mg) and semaglutide 1 mg were achieved. Efficacy estimand. MMRM analysis, mITT population (efficacy analysis set). Data presented are LS mean. Tirzepatide vs. semaglutide 1 mg at 40 weeks. HbA1c=glycated hemoglobin; LS=least squares; mITT=modified intent-to-treat; MMRM=mixed model for repeated measures.
HbA1c goals
For the secondary endpoint of proportion of patients meeting HbA1c goals, for the goal of an HbA1c of <7%, all treatment arms, including semaglutide, had a high percentage of patients achieving this goal, at 81% for semaglutide 1 mg once weekly and 86%-92% for tirzepatide. However, for an HbA1c goal of <5.7%, only 20% of patients receiving semaglutide 1 mg once weekly achieved this goal compared with 51% of patients receiving tirzepatide 15 mg once weekly. (Figure 4a and Figure 4b).
Moreover, looking at 7-point self-monitored blood glucose, all of the arms showed a downward shift, but tirzepatide treatment was associated with greater reductions in daily mean glucose, pre-meal daily mean glucose, and 2-hour post-meal glucose compared with semaglutide.
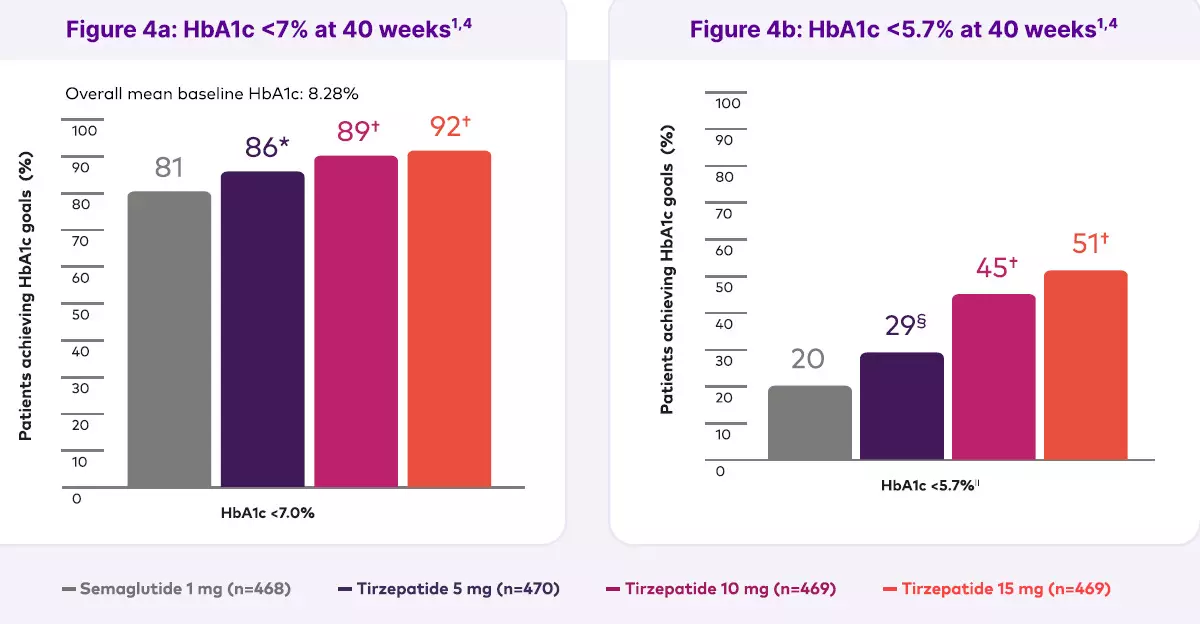
*P<0.05 vs. semaglutide 1 mg for superiority, adjusted for multiplicity. †P<0.001 for superiority vs. semaglutide 1 mg, adjusted for multiplicity.1§P<0.001 compared to semaglutide 1 mg, not adjusted for multiplicity. IINormoglycemia is defined by an HbA1c <5.7%. Efficacy estimand: estimated means, logistic regression, mITT population (efficacy analysis set). Tirzepatide vs. semaglutide 1 mg at 40 weeks.
HbA1c=glycated hemoglobin; mITT=modified intent-to-treat.
Superior mean weight reduction
In addition to the superior glycemic outcomes, tirzepatide was also shown to be associated with superior mean weight reductions over semaglutide at Week 40, with tirzepatide 15 mg delivering double the weight reduction of semaglutide 1 mg, at 12.4 kg, equating to around a 13% weight-loss, compared with 6.2 kg (6.7%). (Figure 5)
Importantly, these significant weight reductions from baseline over 40 weeks with tirzepatide were observed as early as Week 4, and there was no plateau over the course of the study. (figure 6)
The SURPASS-2 study also looked at the proportions of patients reaching weight loss targets of at least 5%, 10% and 15%.
A weight loss of 5% would be considered a really important outcome in a weight-loss trial, which this was not; it is a Phase III glycemic control trial.
Yet in this trial, 58% of patients receiving semaglutide 1 mg once weekly achieved a weight loss of 5%, and 86% of those receiving the highest dose of tirzepatide achieved a weight loss of 5%. When looking at weight loss, 9% of patients achieved 15% weight loss with semaglutide 1 mg once weekly compared with 40% of those receiving the 15 mg once-weekly dose of tirzepatide.
Plotting reduction in BMI shows that while there were reductions with semaglutide, there were relatively greater, dose-dependent reductions seen with tirzepatide, and again we see greater reductions in waist circumference, seeing around a 10 cm reduction in waist circumference with tirzepatide 15 mg once weekly.
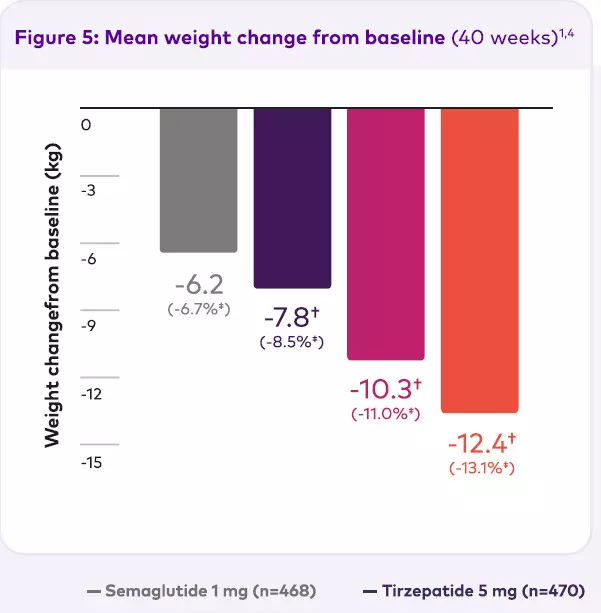
†P<0.001 vs. semaglutide 1 mg for superiority, adjusted for multiplicity. ‡Percentage change from mean weight at baseline.Percentage of weight loss was an approximate calculation of the LS mean for change from baseline divided by the mean baseline value. Efficacy estimand. MMRM analysis, mITT population (efficacy analysis set). Data presented are LS mean. Tirzepatide vs. semaglutide 1 mg at 40 weeks. Tirzepatide is not indicated for weight management. In clinical trials, weight change was a secondary endpoint.1 LS=least squares; mITT=modified intent-to-treat; MMRM=mixed model for repeated measures.
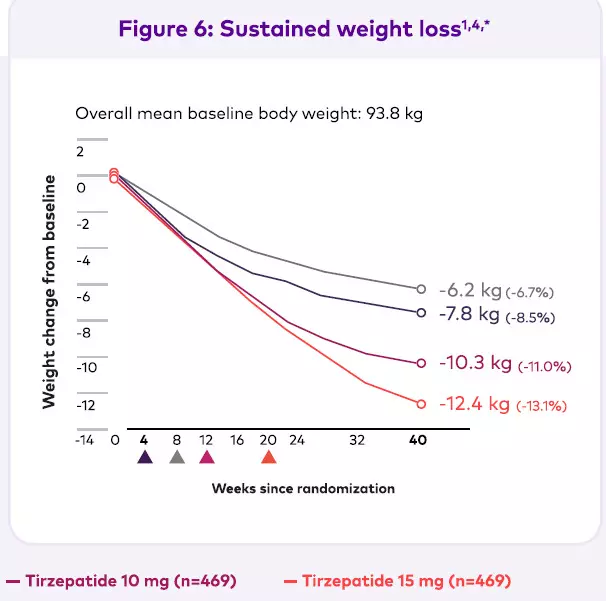
*In clinical trials, weight change was a secondary endpoint.1 Triangles indicate the times at which the maintenance doses of tirzepatide (5 mg, 10 mg, or 15 mg) and semaglutide 1 mg were achieved. Efficacy estimand. MMRM analysis, mITT population (efficacy analysis set). Data presented are LS mean. Tirzepatide vs. semaglutide 1 mg at 40 weeks. LS=least squares; mITT=modified intent-to-treat; MMRM=mixed model for repeated measures.
Beyond weight and glucose
It is important to look at markers beyond weight and glucose. Regarding lipid profiles in patients receiving tirzepatide or semaglutide in the SURPASS-2 trial, there were reductions in triglycerides that were greater with tirzepatide than semaglutide, as well as improvements in high-density lipoprotein cholesterol and significant reductions in very low-density lipoprotein cholesterol.
Tolerability
There were increases seen in gastrointestinal adverse events across all study arms with these incretin-based therapies, but there were no notable differences between tirzepatide and semaglutide. Overall, for gastrointestinal adverse effects, this figure was around 40% for tirzepatide 5 mg, 46.1% and 44.9% for tirzepatide 10 mg and 15 mg once weekly, respectively, compared with 41.2% for semaglutide 1 mg once weekly (Table 2).
Specifically, in terms of the patterns of nausea, vomiting and diarrhea, these increased across all arms at times of titration and tended to reduce over time, and most events were mild to moderate.
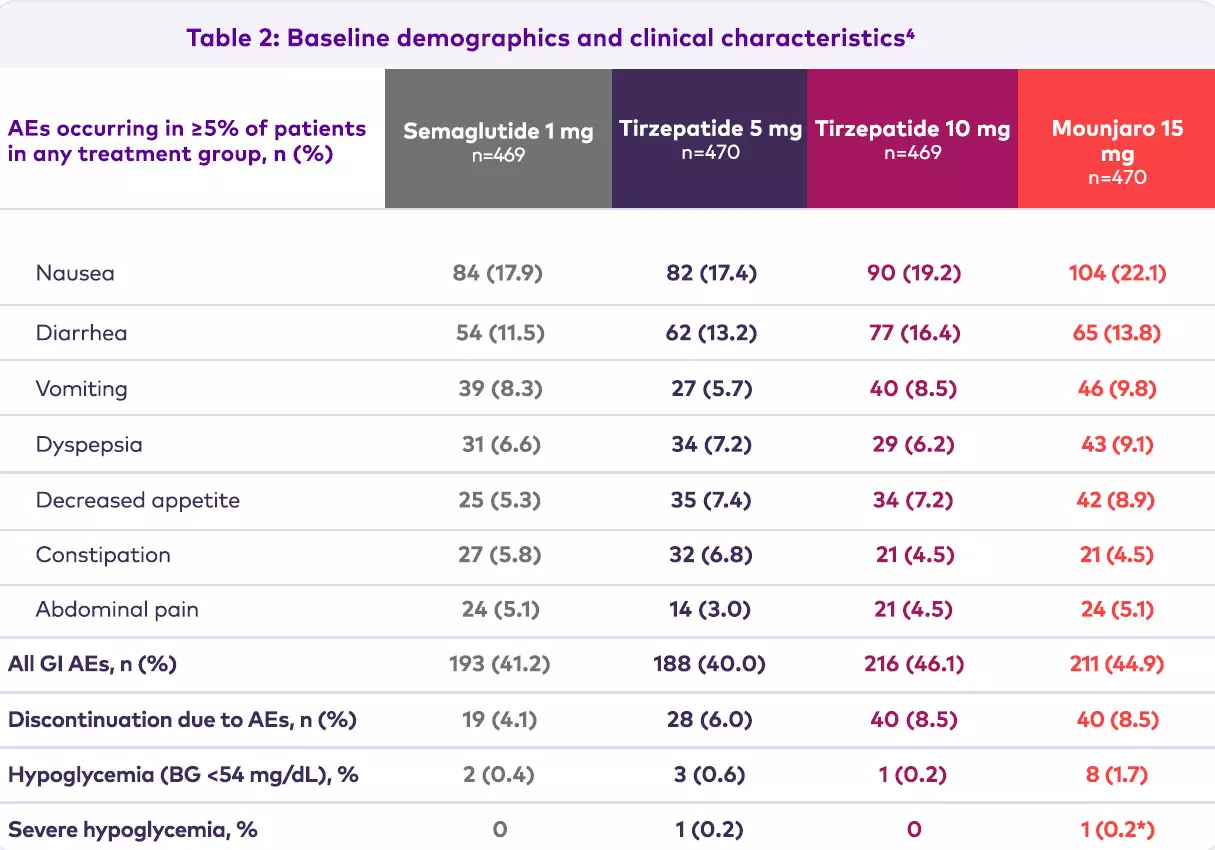
mITT population. No clinically relevant changes in mean calcitonin levels were observed, and no cases of medullary thyroid cancer were reported. *This patient had a hypoglycemic event that was not considered by the investigator to be severe, but it was reported as a serious adverse event. Clinically significant hypoglycemia (BG <3.0 mmol/L [<54 mg/dL] or severe hypoglycemia [requiring the assistance of another person]) occurred in 10–14% (0.14 to 0.16 events/patient year) of patients when tirzepatide was added to sulphonylurea and in 14–19% (0.43 to 0.64 events/patient year) of patients when tirzepatide was added to basal insulin. The rate of clinically significant hypoglycemia when tirzepatide was used as monotherapy or when added to other oral antidiabetic medicinal products was up to 0.04 events/patient year. In Phase 3 clinical studies,10 (0.2%) patients reported 12 episodes of severe hypoglycemia. Of these 10 patients, 5 (0.1%) were on a background of insulin glargine or sulphonylurea who reported one episode each.
AE = adverse event; BG = blood glucose; GI = gastrointestinal; mITT = modified intent-to-treat.
Hypoglycemia
Rates of hypoglycemia in this trial were low, and there were very few episodes of severe hypoglycemia. Looking at adverse events of special interest, these were low and did not appear to be different between semaglutide and tirzepatide (Table 2).
Blood pressure and heart rate
There were reductions in both systolic and diastolic blood pressure in the SURPASS-2 trial and an increase in heart rate, which were similar with tirzepatide and semaglutide.
Conclusions
In the SURPASS-2 trial in people with T2D inadequately controlled on metformin monotherapy, once-weekly tirzepatide, a dual GIP/GLP-1 receptor agonist, demonstrated4:
- Superior and clinically meaningful improvements in glycemic control.
- Significant reduction in body weight.
- Achievements of HbA1c reflecting almost normoglycemia (<5.7%) in up to 51% of participants.
- Low risk of hypoglycemia (blood glucose <54 mg/dL) or severe hypoglycemia.
References
1. Tirzepatide India Prescribing Information | Updated March 2025
2. Nauck MA, Quast DR, Wefers J, et al. GLP-1 receptor agonists in the treatment of type 2 diabetes - state-of-the-art. Mol Metab. 2021;46:101102.
3. Christensen M, Vedtofte L, Holst JJ, et al. Glucose-dependent insulinotropic polypeptide: a bifunctional glucose-dependent regulator of glucagon and insulin secretion in humans. Diabetes. 2011;60(12):3103-9.
4. Frías JP, Davies MJ, Rosenstock J, et al. Tirzepatide versus semaglutide once weekly in patients with type 2 diabetes. N Engl J Med. 2021;385(6):503-15.
5.European Medicines Agency. Ozempic. Summary of Product Characteristics 2018 [updated February 2022]. Available from: https://www.ema.europa.eu/documents/productinformation/ozempic-epar- product-information_en.pdf product-information_en.pdf.

Disclaimer:
This material (including any link) is intended solely for the use of the recipient(s) and may contain confidential information. Any unauthorized review, use, disclosure, copying, or distribution is strictly prohibited. If you are not the intended recipient, please notify the sender immediately and destroy all copies of the material. This material is being provided to healthcare professionals for their guidance and use. Nothing on this website/microsite/material should be construed as giving medical advice or making recommendations regarding any health-related decision or action.
Mounjaro®, KwikPen® and Lilly are registered trademarks of Eli Lilly and Company. To be sold by retail under prescription of Endocrinologist or Internal Medicine Specialists only. For adverse events and safety reporting, please reach out to: mailbox_in-gps@lilly.com For any additional information related to Lilly products, please reach out to: queries_in-medinfo@lilly.com. For further Information about Lilly and Lilly products please contact us at the below address: Plot 92, Sector 32 Gurgaon, Haryana, 122001 India Ph.: +91-124-4753000/01 | www.lilly.com/in.
PP-TR-IN-0948 | 28 January 2026
Eli Lilly and Company. All rights reserved.