From Psoriasis to Psoriatic Arthritis: Strategies for Early Risk Modification



Key Summary The transition from psoriasis to psoriatic arthritis (PsA) is driven by several modifiable risk factors, including obesity, severe skin involvement, and specific lesions on the scalp and nails. 1-5 Research indicates that early intervention with biologics, particularly IL-17A inhibitors like Copellor (ixekizumab), can significantly lower the risk of this progression,...
Key Summary
The transition from psoriasis to psoriatic arthritis (PsA) is driven by several modifiable risk factors, including obesity, severe skin involvement, and specific lesions on the scalp and nails. 1-5 Research indicates that early intervention with biologics, particularly IL-17A inhibitors like Copellor (ixekizumab), can significantly lower the risk of this progression, with studies showing these treatments achieve the lowest prevalence of PsA compared to other classes. 6-9 Because even a six-month delay in diagnosis can lead to permanent joint erosion, clinicians are urged to use screening tools like the PEST to ensure prompt referral and to adopt a holistic, multidisciplinary approach that prioritizes high clearance in both dermatological and joint domains. 6
Optimizing Psoriatic Arthritis Prevention by Managing Psoriasis Risk Factors
Progression to PsA is influenced by several identified risk factors. Long-term indicators (typically appearing 7–12 years before onset) include obesity, genetic history, and specific disease locations such as the scalp and nails, as well as severe overall skin involvement. 1-4 Short-term warning signs (1–3 years before onset) often manifest as joint pain (arthralgia) and subclinical inflammation of the entheses or synovium. 5 Effective management of these initial PsO symptoms is considered a vital step in modifying the risk of developing joint disease.
Utilizing Biological Therapies to Lower the Likelihood of Psoriatic Arthritis Development
Research indicates that treatment with biologics can successfully delay or reduce the transition to PsA. 6,7 Real-world data suggest that IL-17A inhibitors are particularly effective in this regard; patients treated with this class showed a lower risk of progression compared to those on IL-23 inhibitors. Specifically, one large study found that patients on IL-17 inhibitors had the lowest prevalence of PsA (1.9%) compared to those on TNF inhibitors (8.8%) or IL-23/IL-12 inhibitors (6.1%). 7
Core Insights and Performance Metrics of Copellor (ixekizumab)
Copellor (ixekizumab) addresses the primary risk factors for PsA by providing high clearance rates in the skin, 8,9 scalp, and nails. 10
- Skin Clearance: Approximately 40% of patients achieve complete skin clearance (PASI 100) by Week 12, a result that remains stable through one year of treatment (figure 1). 8,9
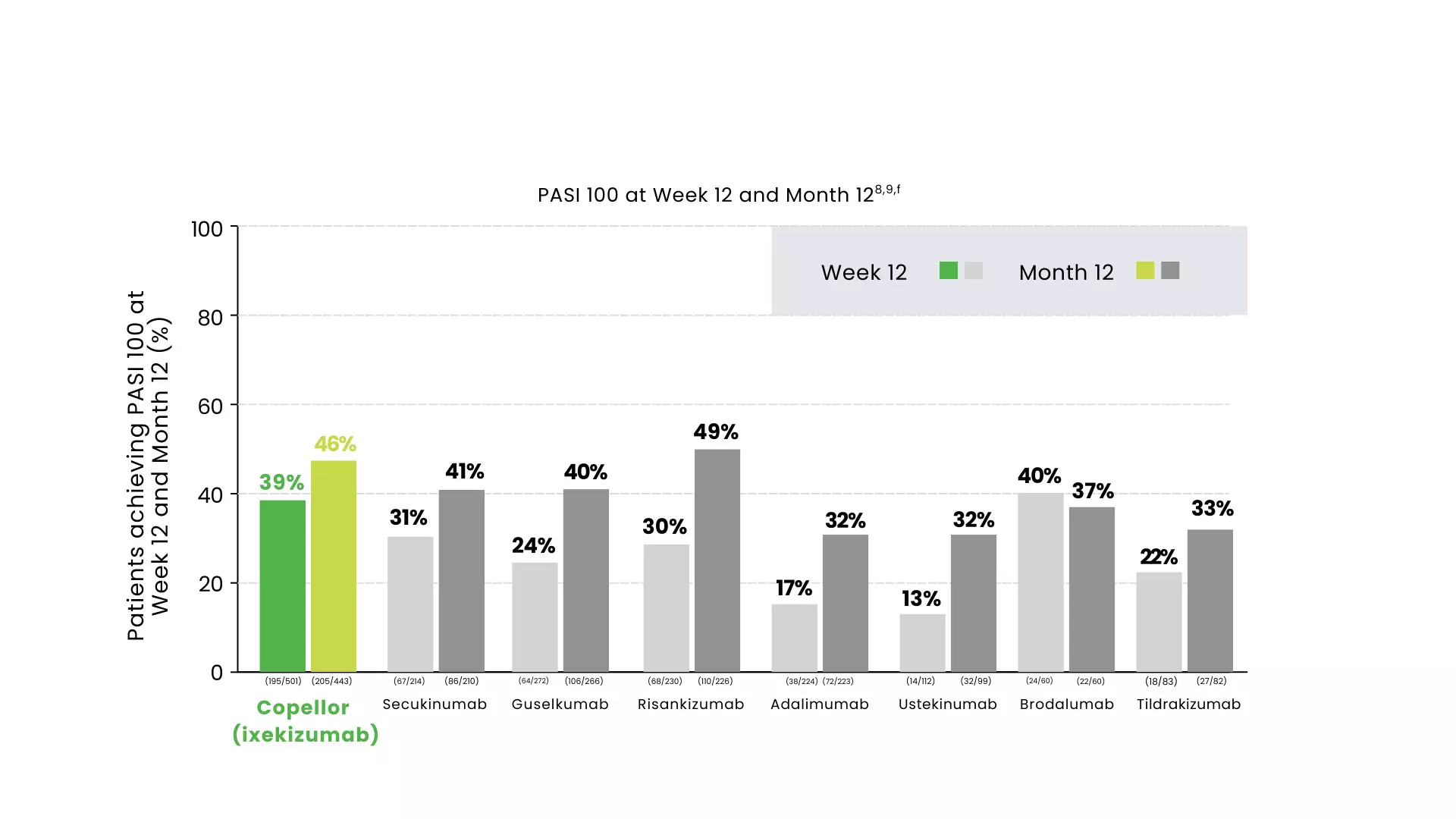
Figure 1: PASI 100 at Week 12 and Month 12
- Scalp and Nail Efficacy: Copellor (ixekizumab) shows superior results in difficult-to-treat areas, with roughly 70% of patients achieving clearance in both scalp and nails by Week 12 (figure 2 and 3). 10
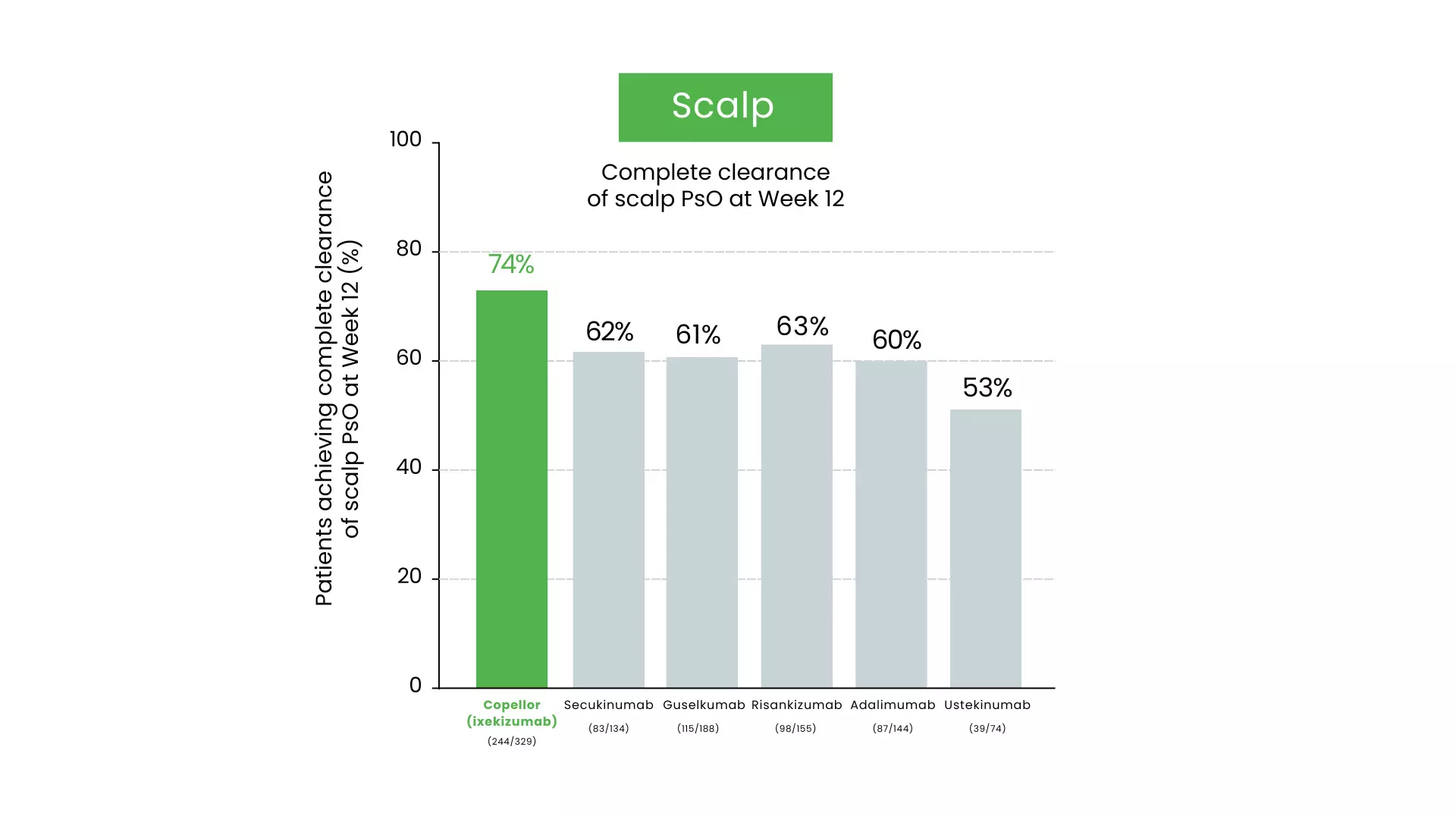
Figure 2: Complete clearance of scalp PsO at Week 12
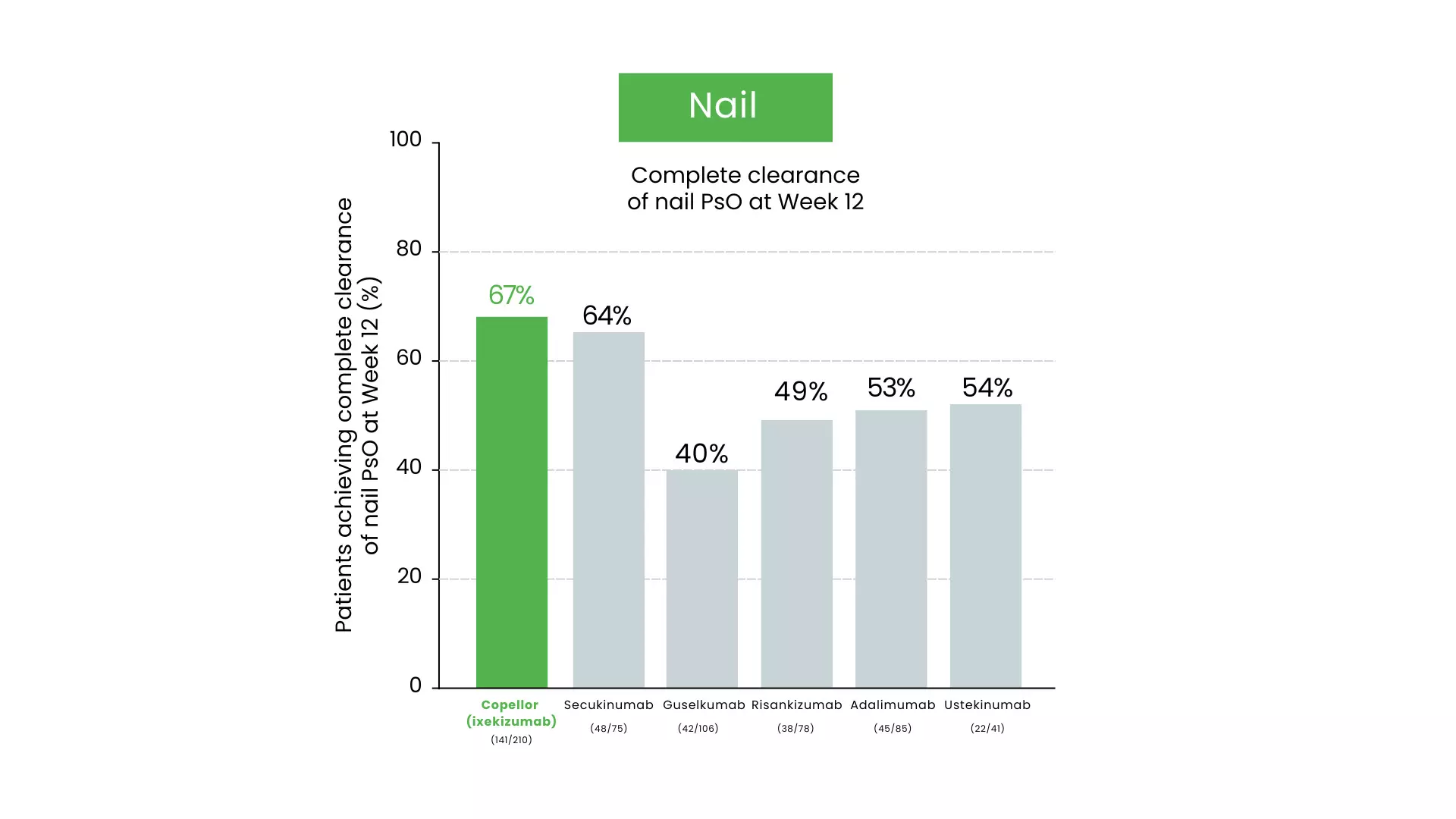
Figure 3: Complete clearance of Nail PsO at Week 12
- Long-term and Comparative Results: By Year 5, scalp clearance reaches 87% and nail clearance reaches 77%. Additionally, network meta-analyses show Copellor (ixekizumab) has the highest probability of achieving complete nail resolution compared to other biologics like bimekizumab and guselkumab. 11-13
The Critical Need for Timely Detection and Specialty Consultation
Early identification is paramount because even a six-month delay in diagnosis can lead to irreversible joint erosion and impaired physical function. 14-16 Dermatologists are encouraged to use validated screening tools like the PEST; a score of 3 or higher necessitates an immediate referral to a rheumatologist to prevent long-term damage. 6
Comprehensive Management of Both Dermatological and Joint Symptoms
For patients who have already transitioned to active PsA, a dual-domain treatment approach is required to improve quality of life. 17 Copellor (ixekizumab) has demonstrated balanced efficacy across both joints and skin. In head-to-head trials against adalimumab, significantly more patients on Copellor (ixekizumab) achieved the combined goal of ACR50 (joint improvement) and PASI 100 (skin clearance) at both 24 and 52 weeks.18 Real-world studies further support these findings, showing significant improvements in Clinical Disease Activity Index (cDAPSA) and Body Surface Area (BSA) scores over 12 months (figure 4).
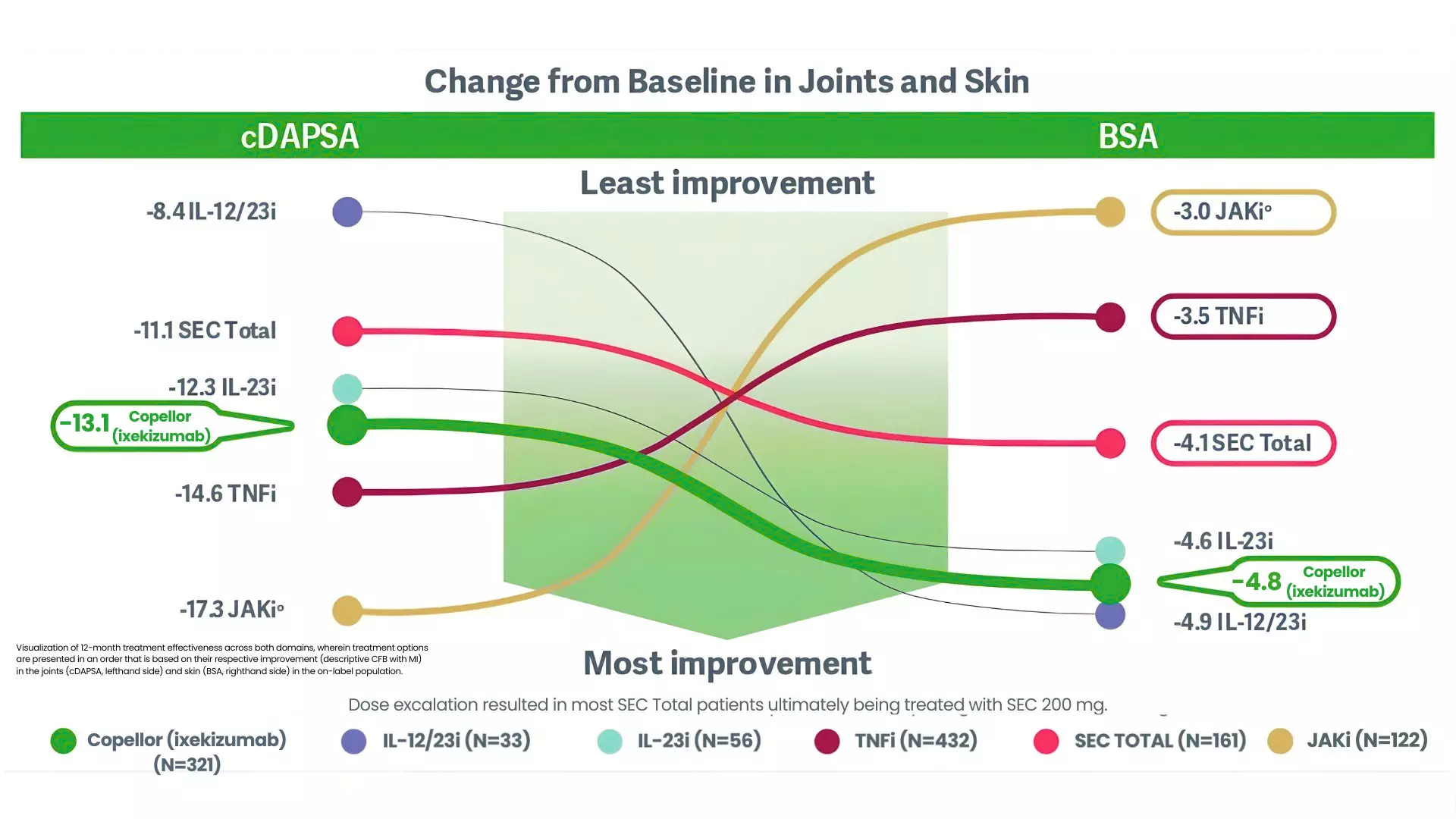
Figure 4: Change from Baseline in Joints and Skin
Adopting an Integrated Strategy for Managing Psoriatic Disease
The complex nature of psoriatic disease requires a multidisciplinary and holistic approach. 2 Treating PsO effectively before the onset of joint symptoms is a proactive strategy to reduce progression. 6,7 Clinicians may choose therapies that offer proven guidance across multiple domains to ensure optimal outcomes for patients at risk of, or currently living with, active PsA. 6-13
References: 1. Errichetti E, Zabotti A. Dermatol Ther (Heidelb). 2024;14(1):1–3. 2. Zabotti A, et al. Ann Rheum Dis. 2023;82(9):1162–1170. 3. Wilson FC, et al. Arthritis Rheum. 2009;61(2):233–239. 4. de Vlam K, et al. Acta Derm Venereol. 2014;94(6):627–634. 5. Zabotti A, et al. RMD Open. 2024;10(2):e004314. 6. Pinter A, et al. Presented at: European Academy of Dermatology and Venereology Congress 2025. 17–20 September 2025, Paris, France. 7. Floris A, et al. Rheumatology (Oxford). 2025;64(3):1131–1137. 8. Pinter A, et al. J Eur Acad Dermatol Venereol. 2022;36(11):2087–2100 (+suppl). 9. Pinter A, et al. Dermatol Ther (Heidelb). 2024;14(6):1479–1493 (+suppl). 10. Piaserico S, et al. Front Med (Lausanne). 2023:10:1185523 (+suppl). 11. Blauvelt A, et al. J Am Acad Dermatol. 2021;85(2):360–368. 12. Reich K, et al. J Dermatolog Treat. 2017;28(4):282–287. 13. van de Kerkhof P, et al. J Eur Acad Dermatol Venereol. 2017;31(3):477–482. 14. Tillett W, et al. Ann Rheum Dis. 2013;72(8):1358–1361. 15. Ocampo DV, Gladman D. F1000Res. 2019;8. F1000 Faculty Rev-1665. 16. Haroon M, et al. Ann Rheum Dis. 2015;74(6):1045–1050. 17. Kavanaugh A, et al. Ann Rheum Dis. 2019;78(9):1215–1219. 18. Reich K, et al. Dermatol Pract Concept. 2022;12(2):e2022104.
Disclaimer: Some molecules/drugs may not be approved in India.
CMAT-16366 | 03/03/2026
Eli Lilly and Company (India) Private Limited
For further Information about Lilly and Lilly products please contact us at the below address: Plot 92, Sector 32 Gurgaon, Haryana, 122001, India Ph.: +91-124-4753000/01 | www.lilly.com/in
For adverse events and safety reporting, please reach out to: mailbox_in-gps@lilly.com | For any additional information related to Lilly products, please reach out to: queries_in-medinfo@lilly.com.
This material (including any link) is intended solely for the use of the recipient(s) and may contain confidential information. Any unauthorized review, use, disclosure, copying, or distribution is strictly prohibited. If you are not the intended recipient, please notify the sender immediately and destroy all copies of the material. The information provided in this section is intended solely for the use of registered medical practitioner. This material is being provided to healthcare professionals only for their guidance and use. Nothing on this website/microsite/material should be construed as giving medical advice or making recommendations regarding any health-related decision or action.
© 2026 Eli Lilly and Company